

Your Biggest Questions, Answered
ART – Assisted Reproductive Technology
BCP – Birth Control Pill
BETA – Blood Test for Pregnancy after Transfer
DET – Dual Embryo Transfer
DPT – Days Post Transfer
ED – Egg Donor
EDD – Estimated Due Date
FET – Frozen Embryo Transfer
GC – Gestational Carrier
HCG – Human chorionic gonadotropin
HPT – Home Pregnancy Test
HSC – Hysteroscopy
IF / IM – Intended Father / Intended Mother
IP – Intended Parent
IVF – In Vitro Fertilization
LMP – Last Menstrual Period
OBGYN – Obstetrics & Gynecology
P4 – Progesterone
PBO – Pre Birth Order
PIO – Progesterone in Oil
RE – Reproductive Endocrinologist
SET – Single Embryo Transfer
SubQ – Subcutaneous Injections
TS – Traditional Surrogate
VBAC – Vaginal Birth After Cesarean
You’ve been matched! What’s next? Now, you will travel to your Intended Parents’ clinic for a day or two of medical screening. Your case manager can clarify how many days you will be away from home (if the clinic isn’t near you) so that you can plan accordingly. You can also provide FMS with any blackout dates so that we can work around your schedule, if possible. Some clinics have quick availability, others have quite a wait. Some testing may require that you visit the clinic during a certain week of your menstrual cycle, so it’s important that you keep up with when you start your period each month so we can determine trip dates. You will undergo physical and psychological evaluations to confirm your suitability to be a Gestational Surrogate! During your medical screening appointment, the clinic requires extensive blood tests to check for hormone levels and
infectious diseases. Depending on the lab, it will take 5 – 14 days to receive those results. Your psychological evaluation may have also included a personality test, which may take a week or two for the mental health professional to interpret and approve the results. Once all of this has been
completed, we will receive word from the clinic that you are indeed ready to begin the next step!
LEGAL (approx 2 weeks after Medical Approval)
Now that you’ve been approved by the clinic to be a Gestational Surrogate, we begin the legal phase of your journey! A written contract, covering every scenario and situation imaginable, is necessary to protect you and your Intended Parents’ best interests throughout your journey. Much of the
information included in the contract is taken from the FMS Match Terms you agreed to when creating your profile, but there will be additional topics to review and consider as well. Your FMS case manager will recommend qualified and respected attorneys in your state, from which you can then choose the best one to represent you. The duration it takes for contracts to be signed greatly depends on the availability of your lawyer, and the lawyer representing your Intended Parents.
GETTING YOUR CALENDAR
Unlike “naturally conceived” pregnancies, preparation for IVF/embryo transfer is very planned and exact. Once legal clearance is received, your clinic
will immediately provide you with a calendar. This calendar will outline not only when each appointment will be for the next 4-6 weeks, but also what medications you will be taking each of those days. Your clinic will send prescriptions to their preferred pharmacy, and that pharmacy will then call you to confirm delivery address. Once you receive your medications, your Case Manager will go over the contents of the box and help you verify that you have everything mentioned on your calendar. She can also provide you with tips and tricks on remembering to take each medication, and ways to minimize any discomfort you may experience.
MOCK CYCLE, ERA TESTING, OR ENDOMETRIAL SCRATCH
Not many clinics require these, but they are worth mentioning. Some fertility specialists take extra steps to ensure that they perform testing to maximize success. This may include a “mock cycle” where you take medications and attend monitoring appointments as a test-run before the real thing. In other cases, the doctor may want to obtain a small sample of endometrial tissue during a certain time of your cycle to guide medication administration or to encourage increased blood flow to your lining. Any of this testing would occur the month before a scheduled embryo transfer.
PREPARING FOR TRANSFER
After you begin your next period, you will have your first ultrasound with blood work to ensure that your lining is appropriately thin and
your ovaries are quiet. This appointment, and the ones leading up to embryo transfer, will occur at a fertility monitoring clinic as close
as we can find to your home or work. They will always occur in the early morning, so be sure your work or home schedule permits
these appointments. You will be given a calendar with these dates well in advance for planning purposes. You may be required to take Lupron before or immediately after this appointment, which suppresses natural ovulation.
Regardless of the protocol, you will take medications for 3-5 weeks leading up to the big moment – embryo transfer!Approximately 2
weeks after beginning estrogen, you will have 1-2 more ultrasounds to check lining thickness. Once it is thick enough, your transfer date will be confirmed and travel will be booked!
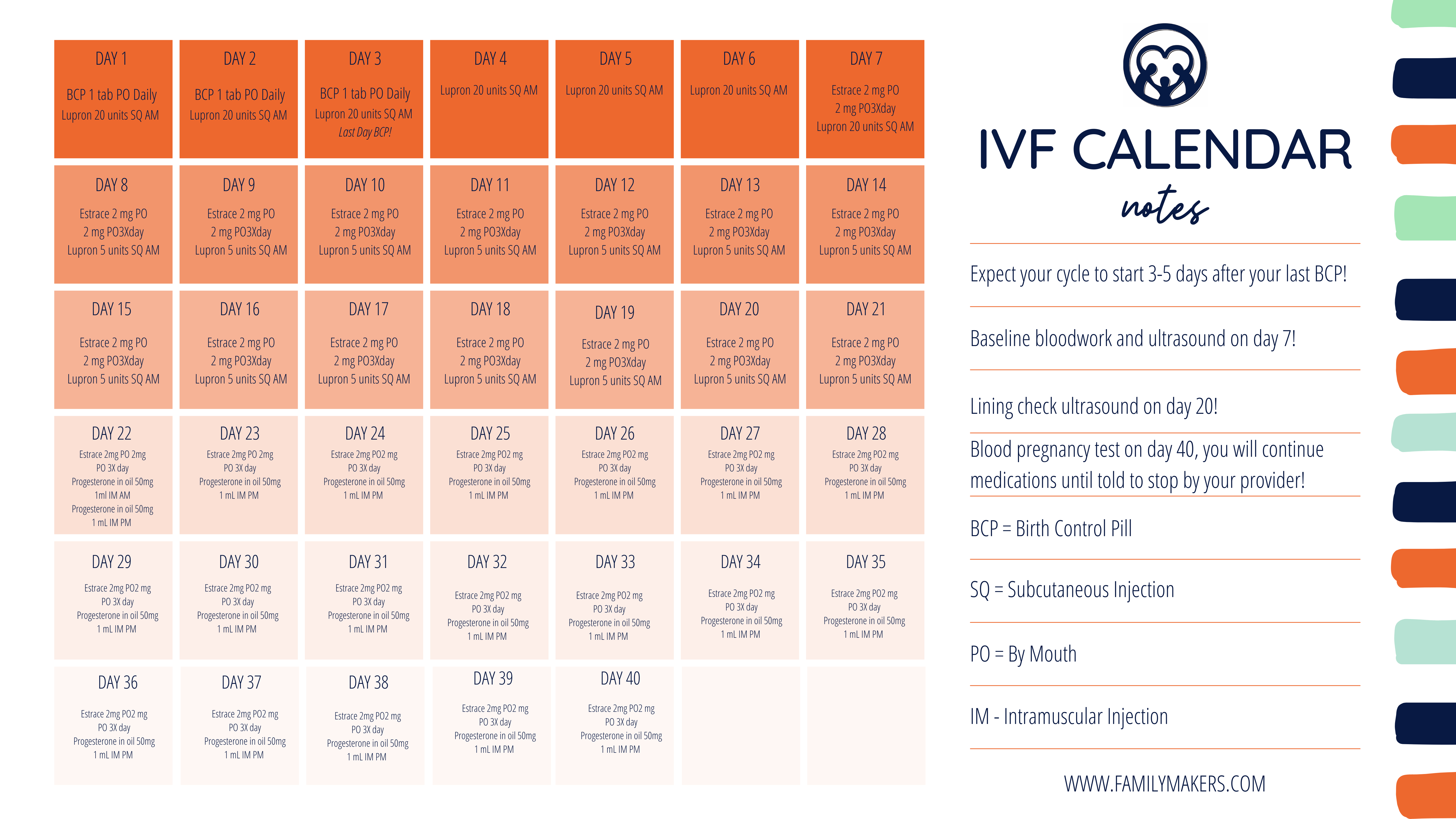
Be sure to check out the sample IVF Calendar on this page!
IT’S TRANSFER DAY!
The day we have all been waiting for is here, and you are probably very excited and nervous! Transfers typically happen between 10am
– 2pm at most clinics, which means you will arrive the night before if traveling to your IPs’ clinic. Get a good night’s sleep and be ready
to arrive with a comfortably full bladder at a time assigned by your IVF nurse. Most IPs attend embryo transfer, and most accompany
their GCs into the Transfer Room when the time comes. There will be a TV screen, and you can all watch together as a tiny catheter is
placed into the uterus. Your IPs’ precious little embryo will be on the end, and once it’s released, the catheter will be removed and you
are officially “Pregnant Until Proven Otherwise!”It’s usually a quick process, and then you will be instructed on what activities are allowed or not allowed when it’s over.Some clinics will allow you to resume normal activity, while others require “bedrest.”
TO POAS OR NOT POAS? THAT IS THE QUESTION!
After transfer, the dreaded “2 Week Wait” is now upon us. Except in this case, it is never actually two weeks! You and your IPs will need
to discuss and decide exactly when you should start testing, or if you plan to test at all. Some are compulsive testers – meaning they
begin testing every day, as soon as 4-5 days after embryo transfer, to see if they can see a “Squinter” on a home pregnancy test. Please be very sensitive to your IPs, and follow their wishes regarding whether or not they want to know the results. Many IPs have been through a lot and would rather wait until a true blood test confirms pregnancy, while others may request that testing be done at home so they can “prepare themselves.” It is always a good idea to discuss what they want to know, and when they want to know it, so that no one gets disappointed or hurt during this very stressful week of waiting.
BETA DAY – CONFIRMATION OF PREGNANCY
Approximately 10 days after your embryo transfer, you will go to your monitoring clinic or a local lab in the morning and get a blood draw. This result will determine if you are in the early days of pregnancy or not, and you and your IPs will be provided the results later in the day. 2-3 days later, you will repeat this test to ensure that your levels are rising appropriately.
If your blood results have been rising as they should, you will then be scheduled for an ultrasound 2-3 weeks later. This ultrasound will confirm if there is a viable heartbeat! Some IPs do everything they can to come to this appointment, although others cannot or choose not to. If they cannot attend, you can ask the clinic for a copy of “Baby’s First Picture,” and many will allow you to video the monitor as they measure and listen to the heartbeat! For liability reasons, most will not allow the IPs to video call into the appointment, but you can always ask for clarification.
WEEKS 6-12
At some point between heartbeat confirmation and 12 weeks pregnant, the fertility doctor who has been overseeing your pregnancy will discharge you into the care of your OB or midwife. This is when this pregnancy becomes very much like any other pregnancy, except you will want to be sure to include your IPs in on anything you can. Be sure your provider has any updated insurance information and a signed HIPAA release on file so that your IPs can discuss things with your provider if ever needed. Discuss any testing options your IPs may want to have, including genetic testing like
MaterniT21 and/or an NT scan. These tests are done between weeks 10-13, so it will need to be mentioned at your first or second appointment with your provider.
WEEKS 13-24
This is what we usually consider to be a quiet time, in which we hope that the pregnancy is an uneventful one with a few regular appointments. One important appointment that many IPs want to attend is the “Anatomy Scan,” done at 18-20 weeks, in which your provider will confirm that everything looks normal and growth is on track. Remember to refer to any stipulations regarding termination in your contract, or in the laws of your State, and
attempt to schedule this appointment earlier rather than later in case something unexpected is found. If further testing or a second opinion needs to be pursued, time may be of the essence.
WEEK 24: VIABILITY!
While it’s not exactly 24 weeks for every pregnancy, the 24 week mark is typically what is referred to as “Viability Week.” This means that should the pregnancy end for some unexpected reason, the baby has a fighting chance to survive outside of the womb. This is also the point in which FMS will reach out to your attorneys to begin the Pre-Birth legal process. You will be asked to sign an affidavit stating that you do not intend to claim or parent
your Intended Parents’ baby, while at the same time your IPs’ will be declaring guardianship and parental rights of their baby. Sometimes your
attendance at a hearing is also required, and we can let you know if that situation applies to you in advance.
WEEKS 25 – DELIVERY
While we wait on the courts to sign the Pre-Birth Order (if applicable), FMS will be reaching out to your delivering hospital to prepare them for your upcoming delivery. You and your IPs may also wish to do a hospital tour during one of their visits, which will allow them to see where their baby will be born and ask the hospital staff any questions they have.If your IPs aren’t local, FMS will assist them with a “post-birth plan” to document their
wishes in case they do not make delivery. Hopefully, they will be able to witness the birth of their child and so we encourage you to talk about how you would like that to look like! If you have any special requests, let us know and we can help communicate those wishes to your IPs if you need it.
By the time the baby arrives, we will provide the hospital with legal documents required to complete the birth certificate, insurance information for both you and the baby, advanced directives, financial guarantor paperwork completed, and emergency contact information to reach FMS or attorneys when the time comes.
IT’S SOMEONE’S BIRTHDAY
Delivery day is finally here, either spontaneously or planned, and there is a flurry of activity happening! Many hospitals will accommodate our request for a separate room for your IPs and their baby, so that you can rest and recuperate after a long 9 months of babysitting! If your delivery was uncomplicated, your hospital may allow you to leave within 24 hours – or you can take advantage of the time off by staying! YOU DID IT!!!
If you haven’t already, be sure to join our Family Makers Surrogate FB group if you would like to give and receive support from our other GCs! You can also follow our FMS page on FB and IG, where you will see regular updates and congratulatory posts for you and your IPs once you begin your
journey.
We love updates, bump pics and any news you’d like to share with our followers! The group is Secret, so your case manager can add you.Please remember to refer to your match terms and/or contract regarding sharing information on social media. If you aren’t sure what you can/can’t share, let us know and we’d be happy to clarify for you. Typical guidelines are to refrain from posting identifying info about your IPs, and no photos of their
baby (ultrasounds or delivery) without their permission.
Each clinic has their own preferences for ordering medication, but one thing remains the same. There is usually a two-step process to getting them ordered and refilled when you need them. This two step process can take time – as the pharmacy usually reverifies delivery address with you, and then calls FMS for payment of those meds. Many pharmacies wait until the end of the day to contact us.
When you have one week left of oral or vaginal medications, please go ahead and call in the refill to the pharmacy. When you open your last vial of progesterone in oil (if prescribed), please go ahead and call in the refill. DO NOT WAIT to do this at the last minute, which puts undue stress on everyone. We do our best to answer urgent calls after hours, however we cannot guarantee availability after business hours or on weekends. We have had several GCs in the past scrambling or panicking to get meds because they simply waited too long to order. If you think you’ll forget, set an alarm/event on your phone.
If you have been given a 3-4 week supply, it is simple to calculate when to ask for refills. If you have an adverse reactions to medications prescribed to you, please alert your case manager and your clinic immediately. Do not depend on friends or the online community to tell you if something is concerning.
Birth Control Pills
In addition to avoiding an unplanned natural pregnancy after committing to the Surrogacy process, taking birth control before IVF allows the fertility clinic to control the timing of a Surrogate’s menstrual cycle in preparation for starting medications. Many clinics will recommend starting a birth control as soon as medical screening is scheduled. A sample IVF calendar with birth control pills looks almost identical to one that doesn’t.
Estrogen/Estradiol/Estrace
This hormone will almost always be included in your list of medications, and will be what builds your lining for a little embryo to have a place to grow. While usually prescribed as a pill, it can also be administered in the form of injections or patches.
Lupron/Leuprolide acetate
If you research this one, you’ll see that it’s used for a multitude of treatments. For the purposes of IVF, it suppresses your body’s ability to ovulate short term. This is administered as an injection only.
Doxycycline/Azythromicin/Tetracycline
Antibiotics are prescribed as a preventative measure, and is meant to fight off any underlying infection or bacteria that could interfere with implantation.
Medrol/Methylprednisolone
This steroid may be prescribed right before embryo transfer. It is prescribed to prevent inflammation of the uterine lining and the body’s rejection of the embryo.
Progesterone/Crinone/Prometrium/Endometrin
This hormone is vital and what makes the embryo stick to the uterine wall after it’s been transferred safely into the Surrogate. If pregnancy is achieved, it will be taken for another 8-10 weeks until the placenta can naturally support the baby. While it can be taken as a pill or vaginal suppository, it is most commonly taken as in intramuscular injection once a day.
While it is unexpected, it is not uncommon to experience spotting or bleeding while preparing for embryo transfer. When this happens, it rarely causes an issue but can can be a sign of fluctuating hormone levels that need to be managed. If you experience spotting or bleeding, notify your clinic and case manager immediately.
THE UNEXPECTED: BLEEDING WHILE PREGNANT
Also while unexpected and scary, it is not uncommon to experience spotting or bleeding in the first trimester. While bleeding may be a sign of miscarriage, it is really difficult to tell without having an ultrasound to confirm the origin of the bleeding. IVF increases the risks of sub chronic hematoma (SCH), which are pockets of blood in the uterine lining, and something we see often. Depending on the clinic you are working with, you may be asked to limit physical activity if this happens. Usually, they go away with a little rest and time. If they don’t, then you physician will recommend a plan of action.
It is understandable to panic if you begin bleeding. The very first call you should make if this happens is to your clinic or to your OB, whichever one is managing your pregnancy at that time. If you must leave a message, include when you began bleeding, how long you have been bleeding, and any pain you are experiencing. While waiting for a call back from a nurse or on-call physician, notify your Intended Parents and case coordinator.
You may be instructed to go to the emergency room if symptoms persist, but most providers will instruct you to come in the following day for an ultrasound.If you are in your second or third trimester, you may be instructed to go to L&D for assessment. Rest and hydrate as much as possible in the meantime.
We thoroughly enjoy supporting you and your IPs during your journey, and attempt to be available whenever you need us.For truly urgent matters, we encourage you to always call or text us right away if you need assistance. For questions or concerns that you do not consider urgent, please allow us to reply during business hours, as we do try to unplug a bit to spend time with our families.
Many of our GCs prefer text or FB chat over email, so we ask that you refrain from sending messages between 8pm – 8am EST. If you think you may forget your question or concern by waiting, just send us a quick email and we will respond as soon as possible. If your case manager is out of the office due to illness, vacation or travel, you will receive an automatic response to email notifying you of who your main contact will be while she’s out.
COMMUNICATING WITH YOUR IPS
We hope that your relationship with your IPs is a good one and effortless. However, at any point you feel that communication changes or there is an issue in your relationship with your IPs, please notify us immediately. If you and your IPs text/email a lot, always remember that tone is difficult to interpret when we can’t hear words spoken to us – so many misunderstandings occur because of this. Discuss anything that bothers you with your
case manager and we will work hard to help clear the air and get things back on track.
ESCROW
Your compensation and any funding for reimbursements owed to you is held by a third party, independent and unbiased escrow agent. While we will provide instructions on requesting disbursements yourself, we are always happy to help gather and process documentation or requests if you can’t. You always have real-time access to your escrow account to view past, current and upcoming payments via Google Docs or similar online platform.Please remember that FMS has zero control over what your escrow agent requires when it comes to documentation required to pay what is owed. Escrow follows the instructions laid out in the terms of your contract to the letter, and we cannot override what is required.
While we can advocate for you if it is ever needed, please understand that bills are paid by your Intended Parents or through the escrow account.
FMS does not pay bills to any provider or person directly once the contract with your Intended Parents are signed. We are dedicated to assisting you with denied claims, unpaid bills or additional funding as required in your contract, and will work closely with you to address any issues like that if they arise. However, your Intended Parents are ultimately responsible for any financial costs covered and outlined in your contract.
The Surrogacy Contract, also called a Gestational Carrier Agreement, is a lengthy document outlining all of the terms agreed upon by the Intended Parents and the Surrogate. The contract should be drafted by an attorney experienced in surrogacy that understands all of the complex issues that commonly occur in surrogacy arrangements. The Surrogate should also have independent legal counsel representing her best interests who can ensure that the terms are balanced and fair.
The contract is one of the most important components of the process because it clearly outlines the rights and responsibilities of both parties. The intention of outlining every detail possible is to minimize misunderstandings and conflicts during the journey, while protecting everyone involved. It addresses compensation and benefits owed to the Surrogate, the Surrogate’s medical risks and responsibilities throughout the process, agreement on issues pertaining to medical decisions such as termination and selective reduction, and even expectations regarding communication during and after the process.
When you are approximately 20 weeks pregnant, the attorney will begin to draft the parentage orders to ensure a smooth legal process upon delivery. Your Case Manager will forward you and your Intended Parents a Parentage Worksheet at that time, which will be provided to the attorney drafting the orders.